{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CONTACT US
We would love to speak with you.
Feel free to reach out using the below details.
GET IN TOUCH
HOURS
- Mon-Thu 9:00AM - 5:00PM
- Friday 9:00AM - 12:00PM



At Ayana Medical Dermatology we are proud to be the only practice in South Florida offering the most cutting edge, non-surgical treatment option on the market for hair restoration. Our experts combine this painless treatment with a customized protocol of medical grade products used to stimulate the growth of hair follicles, while improving circulation of blood and nutrients to the scalp.
There are several different types of hair loss, broadly categorized as either scarring or nonscarring. When assessing hair loss, it is important to determine the type and pattern as this will guide the course of treatment and maximize results. Non-scarring alopecia involves an active phase of hair loss, without permanent injury to follicular stem cells, and is thus potentially reversible. Scarring alopecia implies damage to the hair follicles from chronic inflammation, where they have become replaced by thick connective tissue. The progression from early inflammation to long-standing chronic scarring alopecia can be gradual and without a clear distinction, highlighting the importance of early detection and evaluation of hair loss in order to begin treatment before permanent damage to the hair follicles occurs.
Androgenetic alopecia, known as either male or female pattern hair loss, is multifactorial, and results from the influence of both hormonal and genetic factors. The genetic input can come from either parent, both parents, or even without any strong family history of the condition. An increased expression of androgens, hormones such as testosterone and dihydrotestosterone (DHT), lead to changes in hair follicles and hair shafts. In men, high levels of DHT, as well as recently discovered enzymes involved in androgen metabolism, are found within the hair follicles of the scalp, beard and chest.
In women, patterns of androgenetic hair loss often occur during or after puberty, in the perimenopausal period or during menopause, when there are fluctuations of the androgen metabolism, widespread hormonal changes, and an underlying genetic predisposition. It is important to differentiate between an abnormal overproduction of androgens due to an underlying medical condition vs a normal genetic predisposition to the effect of increased circulating androgens within the scalp.
Male pattern hair loss is typically symmetric and progressive, but the specific pattern of areas involved can vary among individuals. Hair thinning can occur on the front or sides of the hairline, as well as on the vertex (top) of the scalp. Female pattern hair loss most commonly involves the crown of the scalp leading to a thinner, sparse part, with or without the front hairline being affected.
All hair follicles cycle through three phases: growing phase (anagen), dying phase (catagen) and shedding phase (telogen). It is typical for as many as 100-150 scalp hairs to shed per day, as up to 10% of scalp hairs are in the telogen phase at any given time. When an abnormally large number of hairs enter into the telogen phase simultaneously, this type of hair loss is called Telogen Effluvium. A myriad of stressors are capable of shifting this hair follicle biological clock – these include metabolic alterations such as pregnancy and childbirth, nutritional deficiencies or crash dieting, emotionally traumatic events such as a death or breakup, or physical stress caused by surgery, car accidents, severe illness or injury.
The shedding occurs approximately 3 months after a definable precipitating event, and the time course for how long shedding persists can individually vary and last as long as 6 months. Telogen effluvium may also be due to certain medications, or rarely, have no discernible cause and persist for many years.
Diagnosis of telogen effluvium involves a thorough history of previous events, medications and supplements, as well as a clinical examination demonstrating thinning scalp hair, an in-office hair pull test, and follicle evaluation. Complete resolution of shedding with eventual hair regrowth is expected, and recovery can occur anywhere from several months to years after the process begins. Many treatments are available to expedite this recovery process and stimulate increased hair growth at a faster rate than what would occur without any intervention.
Alopecia areata is a non-scarring patterned alopecia which presents as circular areas of hair loss. There may be only one to few circular or oval patches affected or the entire scalp or body. Both genetic and environmental factors play a role in developing this condition, which is thought to be an autoimmune disease involving inflammatory T cells surrounding the hair follicles. The peripheral rim of a patch of alopecia areata contains the most actively inflamed hair follicles, and is thus the target zone for treatment with injections.
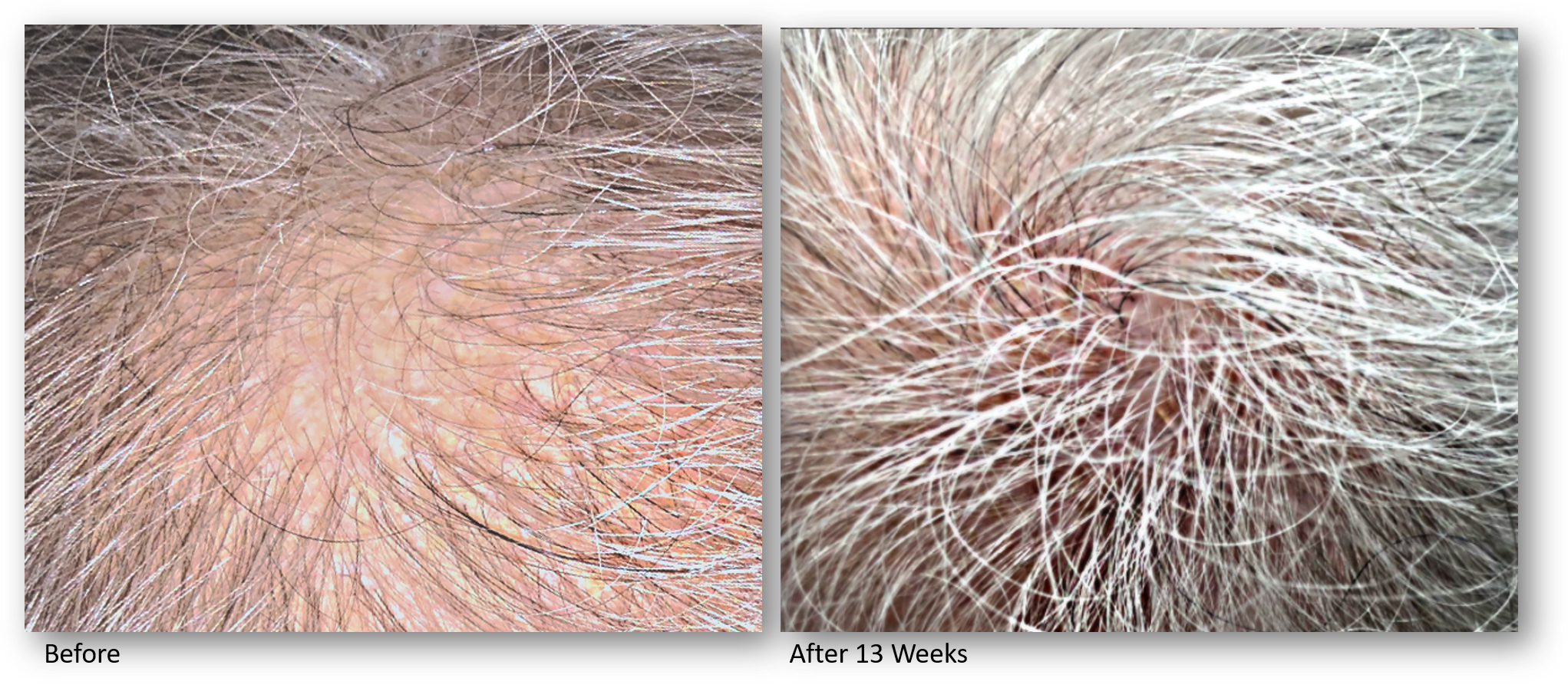
Our Keralase device for scalp revitalization and improved hair quality uses an optimized, intelligent non-ablative fractional laser to promote the rebuilding of healthy scalp skin through a series of gentle yet effective laser treatments. This advanced technology combines laser treatments with a unique and proprietary formulation of a peptide complex precisely created for hair growth. This one-of-a-kind topical serum is a blend of bio-identical growth factors and skin proteins essential for scalp and hair health.
By preconditioning the scalp with fractional laser energy, the skin is able to optimally absorb topical peptides. This painless, in office therapy is a superior alternative to PRP injections, as it requires no blood drawing, no needles, no discomfort and application of a formulation which has been extensively studied and developed inside a nanoliposome carrier to provide the highest concentration of growth factors on the market with the highest absorption rate.





There are several different types of hair loss, broadly categorized as either scarring or nonscarring. When assessing hair loss, it is important to determine the type and pattern as this will guide the course of treatment and maximize results. Non-scarring alopecia involves an active phase of hair loss, without permanent injury to follicular stem cells, and is thus potentially reversible. Scarring alopecia implies damage to the hair follicles from chronic inflammation, where they have become replaced by thick connective tissue. The progression from early inflammation to long-standing chronic scarring alopecia can be gradual and without a clear distinction, highlighting the importance of early detection and evaluation of hair loss in order to begin treatment before permanent damage to the hair follicles occurs.
Androgenetic alopecia, known as either male or female pattern hair loss, is multifactorial, and results from the influence of both hormonal and genetic factors. The genetic input can come from either parent, both parents, or even without any strong family history of the condition. An increased expression of androgens, hormones such as testosterone and dihydrotestosterone (DHT), lead to changes in hair follicles and hair shafts. In men, high levels of DHT, as well as recently discovered enzymes involved in androgen metabolism, are found within the hair follicles of the scalp, beard and chest.
In women, patterns of androgenetic hair loss often occur during or after puberty, in the perimenopausal period or during menopause, when there are fluctuations of the androgen metabolism, widespread hormonal changes, and an underlying genetic predisposition. It is important to differentiate between an abnormal overproduction of androgens due to an underlying medical condition vs a normal genetic predisposition to the effect of increased circulating androgens within the scalp
Male pattern hair loss is typically symmetric and progressive, but the specific pattern of areas involved can vary among individuals. Hair thinning can occur on the front or sides of the hairline, as well as on the vertex (top) of the scalp. Female pattern hair loss most commonly involves the crown of the scalp leading to a thinner, sparse part, with or without the front hairline being affected.
All hair follicles cycle through three phases: growing phase (anagen), dying phase (catagen) and shedding phase (telogen). It is typical for as many as 100-150 scalp hairs to shed per day, as up to 10% of scalp hairs are in the telogen phase at any given time. When an abnormally large number of hairs enter into the telogen phase simultaneously, this type of hair loss is called Telogen Effluvium. A myriad of stressors are capable of shifting this hair follicle biological clock – these include metabolic alterations such as pregnancy and childbirth, nutritional deficiencies or crash dieting, emotionally traumatic events such as a death or breakup, or physical stress caused by surgery, car accidents, severe illness or injury.
The shedding occurs approximately 3 months after a definable precipitating event, and the time course for how long shedding persists can individually vary and last as long as 6 months. Telogen effluvium may also be due to certain medications, or rarely, have no discernible cause and persist for many years.
Diagnosis of telogen effluvium involves a thorough history of previous events, medications and supplements, as well as a clinical examination demonstrating thinning scalp hair, an in-office hair pull test, and follicle evaluation. Complete resolution of shedding with eventual hair regrowth is expected, and recovery can occur anywhere from several months to years after the process begins. Many treatments are available to expedite this recovery process and stimulate increased hair growth at a faster rate than what would occur without any intervention.
Alopecia areata is a non-scarring patterned alopecia which presents as circular areas of hair loss. There may be only one to few circular or oval patches affected or the entire scalp or body. Both genetic and environmental factors play a role in developing this condition, which is thought to be an autoimmune disease involving inflammatory T cells surrounding the hair follicles. The peripheral rim of a patch of alopecia areata contains the most actively inflamed hair follicles, and is thus the target zone for treatment with injections.
Our Keralase device for scalp revitalization and improved hair quality uses an optimized, intelligent non-ablative fractional laser to promote the rebuilding of healthy scalp skin through a series of gentle yet effective laser treatments. This advanced technology combines laser treatments with a unique and proprietary formulation of a peptide complex precisely created for hair growth. This one-of-a kind topical serum is a blend of bio-identitical growth factors and skin proteins essential for scalp and hair health. By preconditioning the scalp with fractional laser energy, the skin is able to optimally absorb topical peptides. This painless, in office therapy is a superior alternative to PRP injections, as it requires no blood drawing, no needles, no discomfort and application of a formulation which has been extensively studied and developed inside a nanoliposome carrier to provide the highest concentration of growth factors on the market with the highest absorption rate.
We would love to speak with you.
Feel free to reach out using the below details.
2140 NE 26th Street Fort Lauderdale, FL 33305
Copyright © 2023 Cherise Mizrahi-Levi DO PA. All rights reserved.